The modern theory of aging





REVIEW
The modern theory of aging, taking into account new data on the role of serotonin in humans and animals
A.P. SIMONENKOV
A.V.Vishnevsky Institute of Surgery, Moscow
The modern theory of aging, taking into account new data on the role of serotonin in humans and animals
A.P. SIMONENKOV
A.V.Vishnevsky Institute of Surgery, Moscow
Explanation of aging mechanism in humans and animals is one of the fundamental problems of all modern science. Understanding of aging process will allow to develop new methods aimed at extending human life. Although many theories of aging have been proposed for recent decades, none of them gives satisfactory explanation of aging mechanism [1–7]. The literature provides different definitions of aging. In our opinion, the most accurate definition is to be found in the Dictionary of physiological terms [8]: “Aging is physiological process accompanied with appropriate age-related changes in the body hereditarily determined and limiting its adaptive and regulatory mechanisms and inevitably leading to senility”. However, despite numerous studies, relation between biochemical and physiological processes that underlie the failure of adaptation and human aging is not completely clear up to now.
The purpose of the study is to demonstrate previously unknown role of serotonin and its receptors in the energy conversion, adaptation, human and animal aging, and also show the opportunity of the development of new pathogenetically reasonable methods in order to extend life span.
Achievements of biology and medicine in recent 30 years open a new view of aging and possibilities of its inhibition. Particularly, our discovery of serotonin deficiency syndrome, contemporary stress and adaptation concept, explanation of the genesis of smooth muscle dysfunction and endogenous vasomotility mechanism, description of serotonin-ferroprotein receptors, improved classification of hypoxic conditions, as well as description of the genesis of age-related and diabetic angiopathy allow us to understand the role of serotonin in human life activity, adaptation and aging [9–14]. The results of our studies have been reproduced in more than 30 medical treatment facilities to confirm their credibility and significance [15–25].
In the study of the aging process you should take into account that all biological objects including man live mainly due to conversion of biochemical energy into electric and mechanical forms interconnected in time and space.
The conversion of energy in different human and animal cells and organs is provided by receptors and their mediators. Physiologists directly state that “the energy of external influence is converted into electric energy as a result of reception processes...” [8]. Moreover, pharmacologists [26] note that “dysfunction of receptors causes cell pathology and death.
In this case, we do not mean any extraordinary cause (e.g., infectious, mechanical ,etc.), but physiological cause, i.e. ordinary aging.”
Since all living organisms grow old, a new theory of aging should explain this process both in unicellular (microbes, etc.) and multicellular organisms including man. Monocellular organisms get nutritive substance from the environment and excrete metabolites in it, i.e. unlike humans they have no systems regulating (limiting) intake of nutritive substances and excretion of metabolites. Human organs are the aggregates of specialized cells, which life activity depends on organ’s blood flow. Delivery of oxygen and nutritive substances into organ cells and also removal of metabolites is regulated by vascular system that depends on the function of smooth muscles (SM) consisting of individual myocytes. Thus, to explain the genesis of SM dysfunction and their recovery (adaptation) is to create the theory of aging of both smooth muscle system and the body as a whole.
Since all living beings are mortal, we can use dichotomic approach and subdivide time of life (from birth to death) in two parts: physiological and non-physiological (pathophysiological) aging. Particularly, according to R.Schmidt & G.Thews [27], aging has usually been considered to be gradual substitution of normal physiological functions by pathological processes. Physiological aging of individual cells and the whole body is accompanied with the decrease of energy conversion process in it.
Under the influence of different external and/or internal factors physiological processes in cells are transformed into pathophysiological (pathological) ones, and aging becomes more intensive (various diseases, sudden death, etc.). Physiological and pathophysiological processes of human aging are interrelated and usually progress according to patterns used by clinicians: health – disease – death; health – disease – heath… – disease – death. Almost all pathological processes developed in human body lead to tissue hypoxia, failure of aerobic energy conversion in tissues, mono- and multiorgan failure. In tissue hypoxia, the failure of energy conversion process is the most pronounced; for example, free energy release in anaerobic conditions is tenfold lower than in the presence of oxygen [27, 28]. All curative measures as well as self-recovery (adaptation) processes are aimed at elimination of tissue hypoxia in affected organ caused by functional and/or morphological reasons. Normalization of energy conversion in tissue leads to suppression of pathological processes and recovery of the organ to the mode of physiological aging.
We revealed previously unknown role of serotonin and its receptors in the genesis of tissue hypoxia as well as in the stress and adaptation genesis that allow us to take a new look at human aging. In humans serotonin is produced by enterochromaffin intestine cells and serotonin producing brain cells. Normal serotonin concentration in blood varies from 20 to 300 µg/L. Serotonin receptors (CR) are mainly located in SM myocytes, CNS, platelets and neutrophils [10, 26, 29].
We disclosed and described endogenous vasomotility mechanisms responsible for tissue metabolism. Periodic smooth muscles (SM) contraction and relaxation (known as “endogenous vasomotility”, “vasomotion”, “vascular motion”, etc.) is going on in the body of healthy people. Endogenous vasomotility (EV) is realized in the following way: serotonin produced by enterochromaffin intestine cells is adsorbed by platelets which release serotonin while passing through microvessels. This serotonin interacts with SR of SM myocytes and converts biochemical energy into electric and mechanical forms causing and supporting automatism and contractile activity of SM of the microvasculature, with typical clinical and electromyographic signs of EV [9 –14].
Tissue metabolism may change under the influence of different stress factors regardless the direction of stressor vector from normal physiological range (to hypo- or hyperoxia, hypo- or hyperthermia, etc.). In other words, in terms of H.Selye [30], every demand to the body (each stressor) changes metabolism of both individual cell and the body as a whole. The change of tissue metabolism leads to emergence of pharmacologically active substances in the blood. The part of this substances bind with SR of SM myocyts, they are SR ligands. SR ligands are subdivided into agonists and antagonists.
Serotonin antagonists interacting with SR cause pathological relaxation (palsy) of SM. Ligands causing pathological contraction (spasm) of SM are called serotonin agonists. Antagonists and/or agonists disturb normal (physiological) energy conversion occurring in SM myocytes during interaction of serotonin with its receptors, which leads to SM dysfunction, failure of EV and the development of tissue hypoxia and organ failure. SR ligands (including physiological and/or pathophysiological metabolites) change serotonin receptors by interacting with them. Serotonin physiological concentration in blood becomes insufficient to provide normal functions of SM and EV that results in relative serotonin deficiency in the body leading to tissue hypoxia. Serotonin deficiency includes the following stages: SR ligands disturb optimal (physiological) conversion of biochemical energy into electric and mechanical forms in SM myocytes (biochemical stage) leading to SM myocyte dysfunction, which is registered by the decrease of EMG and kymogram amplitudes down to the straight line (pharmacological stage); local dysfunction of microvascular SM leads to tissue hypoxia and failure of energy conversion even in the tissues of different organs followed by their insufficiency. SM dysfunction in the whole body leads to vascular insufficiency and/or functional bowel obstruction, total tissue hypoxia and death (clinical stage) [9 –14].
Relative serotonin deficiency cannot be determined using biochemical methods, since one should know not only blood serotonin level but also the degree of myocyte SR degradation. Platelets provide serotonin transportation in blood, therefore low platelet count and local, organ or total SM dysfunction indicate absolute serotonin deficiency which is eliminated by exogenous introduction of serotonin and platelets.
Intravenous and/or intramuscular injection of serotonin adipinate (drug compound) eliminates relative serotonin deficiency, normalizes energy conversion in SM myocytes and recovers SM function.
Treatment of SM dysfunction leads to the recovery of blood flow, elimination of tissue hypoxia, normalization of energy conversion in the organ and recovery of its function. Total 30-year experience of the use of serotonin adipinate in more than 5000 patients with different diseases indicates that its dose depends on the amount of SM myocytes, the degree of their dysfunction and duration of clinical effect achieved [9 – 25].
We should particularly note that smooth muscles consume 100 – 500 times less oxygen than striated muscles to do the same work [21]. In other words, SM contract mainly due to interaction of serotonin with its receptors. Based on this fact, we decided to clarify classification of hypoxic conditions and divided circulatory hypoxia into hypoxia determined by myocardial dysfunction and hypoxia caused by vascular SM dysfunction [12, 13]. According to amended classification, hypoxic conditions include: 1) exogenous hypoxia; 2) respiratory hypoxia; 3) hypoxia caused by myocardial dysfunction; 4) hypoxia caused by dysfunction of vascular smooth muscles; 5) hemic hypoxia; 6) tissue hypoxia; 7) combined hypoxia. This amendment gave us an opportunity to seek diseases, in which tissue hypoxia is manifestation of only SM dysfunction. We supposed that relative serotonin deficiency underlies diabetic and age-related angiopathy (aging). With age vascular intima becomes denser, muscular layer is atrophied, vessels become less flexible and, therefore, not enough able to dilate and contract, i.e. aging of our body is accompanied with failure of EV [3, 10, 14, 27, 31, 32].
This failure of EV is explained by the fact that only free hemoglobin (blood level is 20 – 40 mg/L), physiological metabolite and SR ligand circulating in the blood during the whole life is able to cause degradation of SR and SM dysfunction in humans by interacting with SR of smooth muscle cells [11, 14]. Angiopathy is more pronounced when carbohydrate metabolism is disturbed.
We have shown for the first time [14] that intravenous injection (5 – 10 mg/h) of serotonin adipinate solution in patients with diabetic and age-related angiopathy (n=28) having “diabetic foot” caused increase in SM electric activity with simultaneous decrease of initial tissue hypoxia followed by improvement of wound reparative processes.
Improved microcirculation with subsequent decrease of tissue hypoxia under the influence of only injected exogenous serotonin is another evidence of the validity of our understanding of the genesis of smooth muscle cells dysfunction. The results of this research were later reproduced in other medical care facilities [24, 25, 33].
Understanding of the origin of SM dysfunction and experience of its correction with serotonin allowed us to explain the genesis of stress and adaptation.
According to the literature, myocardial necrotic lesions and small brain cysts are found in apparently healthy persons in 0.9 – 20% of cases (previously, only at postmortal dissection, but now there are intravital findings due to the use of advanced diagnostic techniques). These findings are traces of asymptomatic (“silent”) infarctions and strokes resulted from local failure of microcirculation and activation of endogenous adaptive (antihypoxic, antistress) processes [34 – 36]. Based on previously published and original data, we came to the conclusion that metabolites – SR ligands circulating in the blood cause SM dysfunction and failure of microcirculation with subsequent hemolysis and emergence of free hemoglobin in the blood that activates serotonin release from platelets [11]. This additional endogenous serotonin promotes recovery of energy conversion in SM cells, improves microcirculation, eliminates the area of hypoxia and/or localizes (restricts) necrotized tissue area. Recovery of affected organ’s function only due to the local release of endogenous serotonin is the essence of adaptation. We concluded that exogenous introduction of serotonin in the treatment of tissue hypoxia only simulates increase in the concentration of endogenous serotonin as the material substrate of adaptation. Individual features of adaptation can be explained by different levels of serotonin in people.
On this basis, the following studies have been conducted: patients (45 – 88 years old) (n=53) with different forms of ischemic heart disease having areas of hypokinesis initially passed ultrasound heart examination with registration of heart cavities sizes and myocardial kinetics. Then, the patients were administered intravenous injections of serotonin adipinate for 30 – 60 minutes in the dose of 10 mg dissolved in 200 – 400 mL of physiological solution. The same examination was repeated. Comparative results of these two examinations indicated the increase of contractile activity in hypokinetic myocardial areas accompanied with meaningful increase of stroke volume and ejection fraction [37]. The recovery of contractile activity of the part of cardiac myocytes in myocardial hypokinetic areas with only serotonin may be considered to be functional myocardial “rejuvenation”. In other words, mechanism of endogenous (natural) adaptation was repeatedly reproduced in patients with myocardial hypokinesis. The sole difference from artificial adaptation is that serotonin appears in patients with “silent” myocardial infarctions in the area of disturbed microcirculation from endogenous source – destroyed platelets, whereas for artificial (curative) simulation of adaptation we introduce it externally.
Since the main sign of human aging is the failure of adaptive and regulatory mechanisms (as mentioned above), to explain aging mechanisms we should start with our stress and adaptation concept for different organisms. In our opinion, the following definition of stress is the most grounded for both unicellular organisms and humans:
– in unicellular organisms stress is a result of the failure of optimal energy conversion in the cell under the influence of different factors (stressors) leading to transient impairment of single or several dynamic functions typical of living nature (nutrition, respiration, excretion, irritability, growth, reproduction, mobility);
– in humans stress is a result of the failure of optimal energy conversion in the body under the influence of different factors (stressors) leading to transient impairment of microcirculation and tissue hypoxia in different organs and transient decrease of their function with subsequent activation of endogenous adaptive processes in them and independent recovery of microcirculation, normal tissue metabolism and function.
Appearance of “silent” or symptomatic infarctions in organs (heart, brain, adrenal bodies, etc.) indicates the transition of non-specific stress manifestations into specific ones with typical symptoms of affected organ.
We should pay attention to the fact that biochemical and pharmacological stress stages are common for both individual cells (microbes, etc.) and humans and animals, whereas clinical stage is typical only of humans and animals with developed CNS, and here lies the basic difference between man and unicellular organisms [9].
Contemporary stress and adaptation concept is represented in the Figure. This concept reflects interrelations of stress, tissue hypoxia and adaptation with the development of biochemical and pharmacological stages common for humans and unicellular organisms, and clinical stage specific mainly for humans and animals with developed CNS.
H. Selye [30] also describes manifestations not only general adaptation syndrome, but also local one, which occurs after local trauma, with the development of necrosis, inflammation and wound healing. Experimental studies carried out in cooperation with researchers of Kharkov Medical University have shown that the use of serotonin adipinate improved microcirculation and accelerated healing in rats with stress-associated ulcers caused by 24-hour soft immobilization in supine position, as compared to reference groups [38]. Positive influence of serotonin adipinate on the wound healing in patients and experimental animals has also been reproduced by other researchers [14, 20, 22—25, 33].
Life of biological objects is continuous dynamic process of the transformation of physiological processes (under the influence of various stress factors) into pathophysiological ones, which, in turn, launch material mechanisms of adaptation recovering them into the area of normal physiological processes. Stress and adaptation processes are interrelated and repeatedly transfer into each other not only during human life but sometimes within several minutes or hours. By its nature, the very process of life is dynamics of these transitions; therefore, they cannot be studied separately. Here we have an instance of the philosophic law of the unity and struggle of opposites.
The studies of the role of serotonin and its receptors in life activity of humans and animals indicate that due to quantitative accumulation of serotonin and SR during ontogeny their interaction results in the first process of energy conversion leading to initial contractions of smooth muscles and heart and initial electric activity of brain followed by maintaining their functions throughout the whole life [39, 40]. Here we have an instance of the philosophic law of transformation of quantity into quality.
The failure of physiological interaction between serotonin and SR under the influence of exogenous and/or endogenous SR ligands leads to the impairment of optimal energy conversion primarily in smooth muscle cells and then in organs and tissues caused by hypoxic conditions.
In conditions of tissue hypoxia additional amount of pathophysiological metabolites, myocyte SR ligands, enter the blood, increase and enlarge the area of tissue hypoxia leading to dysfunction of the organ affected, single or multiple organ failure.
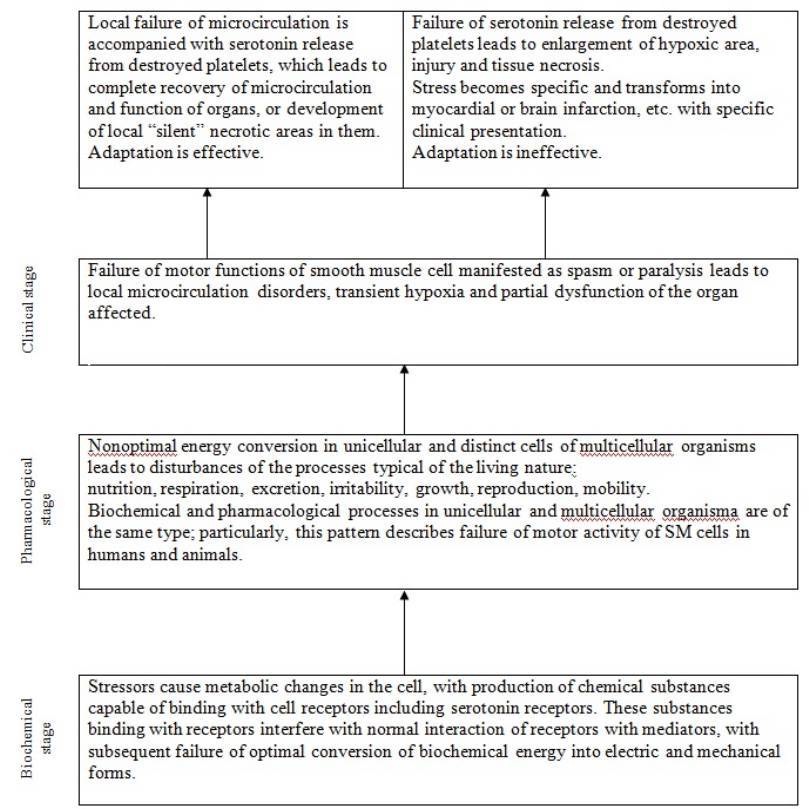
The pattern of interrelations between stress, tissue hypoxia, adaptation and their stages
Exogenous serotonin introduction normalizes disturbed SM function, eliminates tissue hypoxia, optimizes energy conversion in tissues and organs and recovers their function.
Using serotonin in clinical practice we eliminate tissue hypoxia, recover disturbed adaptive processes and therefore prevent separate organs and the whole body from age-related dysfunction maintaining its functional capabilities. The aging process can be presented in the following way: physiological metabolites being SR ligands are produced in the body during life; they disturb optimal energy conversion in SM cells; microvascular SM dysfunction leads to the failure of endogenous vasomotility (EV) and tissue hypoxia.
Tissue hypoxia results in the failure of aerobic processes with generation of additional amount of pathophysiological metabolites – SR ligands, which increase and enlarge SM dysfunction and area of disturbed microcirculation. Then, the process is going on according to the patterns of effective and ineffective adaptation as described above.
Thus, we revealed the genesis of adaptation failures and the way of adaptation process and therefore disclosed the abovementioned adaptive and regulatory mechanisms inevitably leading to senility. Accordingly, aging cannot be stopped but it is possible to retard it and recover previous dysfunction of separate organs.
Since all biological objects utilize different types of energy conversion for their activity, sooner or later they will become old and die. In other words, aging is determined by the fact that efficiency factor of every energy conversion is less than 100%, and according to physical laws every system (living or nonliving) converting energy cannot be eternal. In humans and other living beings the efficiency of energy conversion from one type into another one is at least 35% [8, 27, 41].
The understanding of the importance of energy conversion in human aging will allow to develop in future new quantitative methods of measuring the efficiency factor in different body’s structures and processes (receptors, cells, organs, intermolecular interactions, etc.). Particularly, by measuring efficiency of interaction of certain receptors with their mediators one can identify and correct their dysfunction to prevent tissue hypoxia at the earliest stages, with all ensuing consequences. In other words, prevention and treatment of tissue hypoxia is biochemical and pharmacological basis of aging retardation at the levels of distinct organs and the body as a whole. It was impossible to reveal the genesis of stress and adaptation and therefore to give reasonable explanation of aging mechanisms in humans and animals without our new data on the role of serotonin in human and animal body.
The use of serotonin adipinate for the prevention and in the treatment of symptomatic and latent tissue hypoxia in different organs, along with the elimination of morphological causes leading to tissue hypoxia, will allow to slow inevitable process of human aging, extend average life span and maintain mental and physical abilities. As early as in 1997 the President of the Russian Academy of Medical Sciences noted in his address to the State Duma (the lower house of the Russian Parliament) that prevention and treatment of serotonin deficiency syndrome will allow to extend average life span by 20 – 30 years [42] (or even by 30-50 years, according to our data).
Our data do not contradict but only deepen and broaden the present knowledge.
BIBLIOGRAPHY
1. V.I. Dontsov, V.N. Krut’ko & A.A. Podkolzin. Aging: Mechanism and ways to overcome. Moscow, 1997 (in Russian).
2. Short Medical Encyclopedia. Ed. V.I. Pokrovsky. Moscow, 1994 (in Russian).
3. Blood disorders in the elderly. Eds: M.J.Denham & I. Chanarin. Moscow, 1989.
4. O.V. Korkushko, V.Kh. Khavinson, G.M. Butenko & V.B. Shatilo. Peptide preparations of thymus and epiphysis in the prevention of accelerated aging. St. Petersburg, 2002 (in Russian).
5. V.N. Nikitin. The theory of aging. In Book: Biology of aging. Biology of aging, 1982;
153-174 (in Russian).
6. V.V. Skupchenko, N.E. Poverennova, R.M. Balakleets, et al. Geriatric neurology. In Book: Practical geriatrics. Samara, 1995; 318—360 (in Russian).
7. V.V. Frolkis. Aging and senility. In Book: Biology of aging. Biology of aging, 1982;
5-23 (in Russian).
8. Dictionary of physiological therms. Ed. O.G. Gazenko. Moscow, 1987 (in Russian).
9. A.P. Simonenkov & V.D. Fedorov. Modern stress and adaptation concept taking into account new data on the genesis of tissue hypoxia. Herald of the RAMS, 2008; 5:7-15 (in Russian).
10. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. Mechanisms of endogenous vasomotility and microcirculatory smooth muscle deficiency. Herald of the RAMS, 1994; 6:11–15 (in Russian).
11. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. The ability of hemoglobin and mioglobin to cause smooth muscle spasm and accelerate platelets destruction. Description of serotonin-ferroprotein receptors. Herald of the RAMS, 1995; 12:45–51 (in Russian).
12. A.P. Simonenkov. Reasons for the amended classification of hypoxic conditions. Bulletin of experimental biology and medicine, 1999; 2: 146–151 (in Russian).
13. A.P. Simonenkov, V.D. Fedorov, V.M. Kluzhev, et al. The amended classification of hypoxic conditions. Вестн РАМН 2004; 1:46–48 (in Russian).
14. A.P. Simonenkov & V.D.Fedorov. Is chronic serotonin deficiency the basis of diabetic and age-related angiopathy? Bulletin of experimental biology and medicine, 1997; 1:103 – 110 (in Russian).
15. A.B. Gorpinich. Prevention and treatment of postvagotomy and post-resection motor and evacuatory dysfunctions of gastrointestinal tract: Abstract of Doctorate thesis. Moscow, 1997 (in Russian).
16. G.I. Sinenchenko, V.G. Verbitsky & A.V.Kolunov. Endolymphatic infusion of serotonin adipinate in the treatment of postsurgical enteroparesis. Medical Herald of the Ministry of the Interior, 2006; 2: 21-23 (in Russian).
17. I.A. Kozlov, T.V. Klypa, V.Yu. Rybakov & Yu.G. Matveev. The first use of serotonin adipinate for the correction of vascular insufficiency in cardiosurgical patients. Intensive Care Herald, 2006; 1: 7-9 (in Russian).
18. V.A. Lazarenko, A.P. Simonenkov & E.V. Lazarev. The concept of serotonin use in patients with obliterating atherosclerosis of lower limb vessels at the stage of “critical ischemia”. Actual problems of medicine and pharmacy. Kursk, 2001; 307 – 309 (in Russian).
19. V.I. Lupaltsov, L.Ch. Orazkulieva & A.E. Vishnyakov. The experience of serotonin use in combined treatment of atherosclerotic ischemia of lower limbs. Clinical surgery, 2000; 5: 21 – 23.
20. M.Yu. Lebedeva. Pulsed magnetic field and serotonin adipinate in the prevention of aseptic postsurgical wound healing disorders: Abstract of Ph.D. thesis, Moscow, 2006 (in Russian).
21. E.A. Luzhnikov, V.A. Matkevich, A.S. Savina, et al. The influence of serotonin adipinate on cardiovascular system in patients with circulation disorders after acute poisoning by psychotropic drugs. Critical care medicine at the turn of the XXI century. Moscow,1996; 303-305 (in Russian).
22. O.E. Lutsevich, K.E. Mironov, M.Yu. Lebedev, et al. Mexidole, serotonin and NO-containing gas flows in the prevention of festering and stimulation of postsurgical and experimental wounds healing. Digest of clinical medicine, 2006; XI: 86 – 89 (in Russian).
23. K.E. Mironov. Combined treatment of wounds using serotonin, antioxidants and exogenous nitrogen oxide: Abstract of Ph.D. thesis, Moscow 2006 (in Russian).
24. E.V. Prusov, V.T. Krivikhin, A.P. Simonenkov & V.Ya. Shenshin. The use of serotonin adipinate to improve microcirculation and heal postsurgical wounds in patients with diabetic foot syndrome. Digest of clinical medicine, 2007; XVI: 167 – 169 (in Russian).
25. R.N. Tereschenko. The treatment of ischemic lesion of lower limbs in patients with diabetic foot syndrome using serotonin adipinate: Abstract of Ph.D. thesis. Kursk, 2006 (in Russian).
26. P.V.Sergeev, N.L. Shimanovsky & V.I. Petrov. Receptors of physiologically active substances. Volgograd, 1999 (in Russian).
27. Schmidt R. & G. Thews. Human physiology. In 3 volumes. Moscow, 1996.
28. R. Murray, D. Granner, P. Mayes & V. Rodwell. Human biochemistry. Mosdcow,
1993.
29. Reference book of practical physician. Ed. A.I.Vorobiev. Moscow, 1993.
30. Selye G. The stress concept as we see it,1976 In book: New data on hormones and mechanisms of their action. Kiev, 1977.
31. A.M. Chernukh, P.N. Aleksandrov & O.V. Alekseev. Microcirculation. Moscow, 1984.
32. V.I. Kozlov, E.P. Mel’man, E.M. Neyko & B. M. Shutka. Histophysiology of capillaries. St. Petersburg, 1994 (in Russian).
33. L.I. Belikov, E.A. Bobrovskaya, A.B. Gorpinich, et al. The treatment of ischemically determined forms of diabetic foot syndrome. Herald of new medical technologies, 2006; 13: 4: 40–41 (in Russian).
34. E.I. Chazov. Myocardial infarction. Moscow, 1971.
35. Blood circulation diseases: Internal diseases manual. Ed. E.I. Chazov. Moscow, 1997 (in Russian).
36. B.M. Lipovetsky. Infarction, stroke and sudden death. St. Petersburg, 1997 (in Russian).
37. A.P. Simonenkov, V.M. Kluzhev, V.N. Ardashev, V.D. Fedorov, etc. The use of serotonin adipinate to improve contractile activity of hypokinetic myocardial areas. Journal of military medicine, 2002; 1: 31-35 (in Russian).
38. O.Ch. Khadziev, V.I. Lupaltsov, A.P. Simonenkov, et al. Microcirculatory disorders in gastric mucosa in ulcer and serotonin influence on their dynamics. Bulletin of experimental biology and medicine, 2000; 9: 268 – 271 (in Russian).
39. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. Can we consider serotonin receptors to be “receptors of life”? Herald of the RAMS,1995; 6: 27-30 (in Russian).
40. G.A. Buzhikov. Low-molecular regulators of embryonic development. Moscow, 1967.
41. Physics. Large encyclopedic dictionary. Moscow, 1999 (in Russian).
42. V.I. Pokrovsky. The state of medical science: trends and forecast. Russian medical news, 1997; 3: 27 – 33 (in Russian).
Exogenous serotonin introduction normalizes disturbed SM function, eliminates tissue hypoxia, optimizes energy conversion in tissues and organs and recovers their function.
Using serotonin in clinical practice we eliminate tissue hypoxia, recover disturbed adaptive processes and therefore prevent separate organs and the whole body from age-related dysfunction maintaining its functional capabilities. The aging process can be presented in the following way: physiological metabolites being SR ligands are produced in the body during life; they disturb optimal energy conversion in SM cells; microvascular SM dysfunction leads to the failure of endogenous vasomotility (EV) and tissue hypoxia.
Tissue hypoxia results in the failure of aerobic processes with generation of additional amount of pathophysiological metabolites – SR ligands, which increase and enlarge SM dysfunction and area of disturbed microcirculation. Then, the process is going on according to the patterns of effective and ineffective adaptation as described above.
Thus, we revealed the genesis of adaptation failures and the way of adaptation process and therefore disclosed the abovementioned adaptive and regulatory mechanisms inevitably leading to senility. Accordingly, aging cannot be stopped but it is possible to retard it and recover previous dysfunction of separate organs.
Since all biological objects utilize different types of energy conversion for their activity, sooner or later they will become old and die. In other words, aging is determined by the fact that efficiency factor of every energy conversion is less than 100%, and according to physical laws every system (living or nonliving) converting energy cannot be eternal. In humans and other living beings the efficiency of energy conversion from one type into another one is at least 35% [8, 27, 41].
The understanding of the importance of energy conversion in human aging will allow to develop in future new quantitative methods of measuring the efficiency factor in different body’s structures and processes (receptors, cells, organs, intermolecular interactions, etc.). Particularly, by measuring efficiency of interaction of certain receptors with their mediators one can identify and correct their dysfunction to prevent tissue hypoxia at the earliest stages, with all ensuing consequences. In other words, prevention and treatment of tissue hypoxia is biochemical and pharmacological basis of aging retardation at the levels of distinct organs and the body as a whole. It was impossible to reveal the genesis of stress and adaptation and therefore to give reasonable explanation of aging mechanisms in humans and animals without our new data on the role of serotonin in human and animal body.
The use of serotonin adipinate for the prevention and in the treatment of symptomatic and latent tissue hypoxia in different organs, along with the elimination of morphological causes leading to tissue hypoxia, will allow to slow inevitable process of human aging, extend average life span and maintain mental and physical abilities. As early as in 1997 the President of the Russian Academy of Medical Sciences noted in his address to the State Duma (the lower house of the Russian Parliament) that prevention and treatment of serotonin deficiency syndrome will allow to extend average life span by 20 – 30 years [42] (or even by 30-50 years, according to our data).
Our data do not contradict but only deepen and broaden the present knowledge.
BIBLIOGRAPHY
1. V.I. Dontsov, V.N. Krut’ko & A.A. Podkolzin. Aging: Mechanism and ways to overcome. Moscow, 1997 (in Russian).
2. Short Medical Encyclopedia. Ed. V.I. Pokrovsky. Moscow, 1994 (in Russian).
3. Blood disorders in the elderly. Eds: M.J.Denham & I. Chanarin. Moscow, 1989.
4. O.V. Korkushko, V.Kh. Khavinson, G.M. Butenko & V.B. Shatilo. Peptide preparations of thymus and epiphysis in the prevention of accelerated aging. St. Petersburg, 2002 (in Russian).
5. V.N. Nikitin. The theory of aging. In Book: Biology of aging. Biology of aging, 1982;
153-174 (in Russian).
6. V.V. Skupchenko, N.E. Poverennova, R.M. Balakleets, et al. Geriatric neurology. In Book: Practical geriatrics. Samara, 1995; 318—360 (in Russian).
7. V.V. Frolkis. Aging and senility. In Book: Biology of aging. Biology of aging, 1982;
5-23 (in Russian).
8. Dictionary of physiological therms. Ed. O.G. Gazenko. Moscow, 1987 (in Russian).
9. A.P. Simonenkov & V.D. Fedorov. Modern stress and adaptation concept taking into account new data on the genesis of tissue hypoxia. Herald of the RAMS, 2008; 5:7-15 (in Russian).
10. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. Mechanisms of endogenous vasomotility and microcirculatory smooth muscle deficiency. Herald of the RAMS, 1994; 6:11–15 (in Russian).
11. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. The ability of hemoglobin and mioglobin to cause smooth muscle spasm and accelerate platelets destruction. Description of serotonin-ferroprotein receptors. Herald of the RAMS, 1995; 12:45–51 (in Russian).
12. A.P. Simonenkov. Reasons for the amended classification of hypoxic conditions. Bulletin of experimental biology and medicine, 1999; 2: 146–151 (in Russian).
13. A.P. Simonenkov, V.D. Fedorov, V.M. Kluzhev, et al. The amended classification of hypoxic conditions. Вестн РАМН 2004; 1:46–48 (in Russian).
14. A.P. Simonenkov & V.D.Fedorov. Is chronic serotonin deficiency the basis of diabetic and age-related angiopathy? Bulletin of experimental biology and medicine, 1997; 1:103 – 110 (in Russian).
15. A.B. Gorpinich. Prevention and treatment of postvagotomy and post-resection motor and evacuatory dysfunctions of gastrointestinal tract: Abstract of Doctorate thesis. Moscow, 1997 (in Russian).
16. G.I. Sinenchenko, V.G. Verbitsky & A.V.Kolunov. Endolymphatic infusion of serotonin adipinate in the treatment of postsurgical enteroparesis. Medical Herald of the Ministry of the Interior, 2006; 2: 21-23 (in Russian).
17. I.A. Kozlov, T.V. Klypa, V.Yu. Rybakov & Yu.G. Matveev. The first use of serotonin adipinate for the correction of vascular insufficiency in cardiosurgical patients. Intensive Care Herald, 2006; 1: 7-9 (in Russian).
18. V.A. Lazarenko, A.P. Simonenkov & E.V. Lazarev. The concept of serotonin use in patients with obliterating atherosclerosis of lower limb vessels at the stage of “critical ischemia”. Actual problems of medicine and pharmacy. Kursk, 2001; 307 – 309 (in Russian).
19. V.I. Lupaltsov, L.Ch. Orazkulieva & A.E. Vishnyakov. The experience of serotonin use in combined treatment of atherosclerotic ischemia of lower limbs. Clinical surgery, 2000; 5: 21 – 23.
20. M.Yu. Lebedeva. Pulsed magnetic field and serotonin adipinate in the prevention of aseptic postsurgical wound healing disorders: Abstract of Ph.D. thesis, Moscow, 2006 (in Russian).
21. E.A. Luzhnikov, V.A. Matkevich, A.S. Savina, et al. The influence of serotonin adipinate on cardiovascular system in patients with circulation disorders after acute poisoning by psychotropic drugs. Critical care medicine at the turn of the XXI century. Moscow,1996; 303-305 (in Russian).
22. O.E. Lutsevich, K.E. Mironov, M.Yu. Lebedev, et al. Mexidole, serotonin and NO-containing gas flows in the prevention of festering and stimulation of postsurgical and experimental wounds healing. Digest of clinical medicine, 2006; XI: 86 – 89 (in Russian).
23. K.E. Mironov. Combined treatment of wounds using serotonin, antioxidants and exogenous nitrogen oxide: Abstract of Ph.D. thesis, Moscow 2006 (in Russian).
24. E.V. Prusov, V.T. Krivikhin, A.P. Simonenkov & V.Ya. Shenshin. The use of serotonin adipinate to improve microcirculation and heal postsurgical wounds in patients with diabetic foot syndrome. Digest of clinical medicine, 2007; XVI: 167 – 169 (in Russian).
25. R.N. Tereschenko. The treatment of ischemic lesion of lower limbs in patients with diabetic foot syndrome using serotonin adipinate: Abstract of Ph.D. thesis. Kursk, 2006 (in Russian).
26. P.V.Sergeev, N.L. Shimanovsky & V.I. Petrov. Receptors of physiologically active substances. Volgograd, 1999 (in Russian).
27. Schmidt R. & G. Thews. Human physiology. In 3 volumes. Moscow, 1996.
28. R. Murray, D. Granner, P. Mayes & V. Rodwell. Human biochemistry. Mosdcow,
1993.
29. Reference book of practical physician. Ed. A.I.Vorobiev. Moscow, 1993.
30. Selye G. The stress concept as we see it,1976 In book: New data on hormones and mechanisms of their action. Kiev, 1977.
31. A.M. Chernukh, P.N. Aleksandrov & O.V. Alekseev. Microcirculation. Moscow, 1984.
32. V.I. Kozlov, E.P. Mel’man, E.M. Neyko & B. M. Shutka. Histophysiology of capillaries. St. Petersburg, 1994 (in Russian).
33. L.I. Belikov, E.A. Bobrovskaya, A.B. Gorpinich, et al. The treatment of ischemically determined forms of diabetic foot syndrome. Herald of new medical technologies, 2006; 13: 4: 40–41 (in Russian).
34. E.I. Chazov. Myocardial infarction. Moscow, 1971.
35. Blood circulation diseases: Internal diseases manual. Ed. E.I. Chazov. Moscow, 1997 (in Russian).
36. B.M. Lipovetsky. Infarction, stroke and sudden death. St. Petersburg, 1997 (in Russian).
37. A.P. Simonenkov, V.M. Kluzhev, V.N. Ardashev, V.D. Fedorov, etc. The use of serotonin adipinate to improve contractile activity of hypokinetic myocardial areas. Journal of military medicine, 2002; 1: 31-35 (in Russian).
38. O.Ch. Khadziev, V.I. Lupaltsov, A.P. Simonenkov, et al. Microcirculatory disorders in gastric mucosa in ulcer and serotonin influence on their dynamics. Bulletin of experimental biology and medicine, 2000; 9: 268 – 271 (in Russian).
39. A.P. Simonenkov, V.D. Fedorov, A.V. Fedorov, et al. Can we consider serotonin receptors to be “receptors of life”? Herald of the RAMS,1995; 6: 27-30 (in Russian).
40. G.A. Buzhikov. Low-molecular regulators of embryonic development. Moscow, 1967.
41. Physics. Large encyclopedic dictionary. Moscow, 1999 (in Russian).
42. V.I. Pokrovsky. The state of medical science: trends and forecast. Russian medical news, 1997; 3: 27 – 33 (in Russian).


